

The warning was written in British blood. Alberta read it and said "hold my beer."
Full Disclosure - I am the co-chair of the Palliser chapter of Friends of Medicare. I have been involved with them for five years.
Let us start with a number: 1,300. That is how many people died in England every single month last year because they waited too long in emergency departments, often on gurneys in hallways, after a doctor had already said they needed to be admitted but no bed was available.
You can find a link to the report at the bottom of this article.
England has about 57 million people. Alberta has about 5 million. Do the math, and if we had the same death rate here, that would mean 120 Albertans dead every month. Four people a day. From waiting for a bed that never came in time.
But here is the thing: we do not actually know how many people are dying in Alberta ERs because the government will not tell us. The UK has a Royal College of Emergency Medicine that forces the numbers out into the open. They count the bodies and name the problem.
Alberta gives us silence, no data, no transparency, no accountability.
Dr. Paul Parks spoke about a real person in a real ER
Dr. Paul Parks is an emergency doctor in Medicine Hat who has been touring Alberta with Friends of Medicare raising the alarm. On June 6, he shared a story that should make every single person in this province furious.
A patient in their 40s showed up at the University of Alberta Hospital emergency department with severe chest pain and trouble taking a deep breath. In medical terms, they were a CTAS 2, which means very high risk and very high acuity, the kind of patient who should be seen immediately.
The patient waited.
And waited.
And waited.
At hour nine, they messaged Dr. Parks. Not to ask for special treatment or to try to jump the line, but to ask if they should just leave.
They asked if they should just leave.
They asked if it was possible they might have something bad.
They asked if the system had forgotten about them.
While they waited, their blood work and chest X ray results showed up on their phone, and they read the radiologist's report before ever laying eyes on a doctor.
The patient finally saw a doctor at hour 13.
Let's talk about the waiting time board
Hour nine, the screen said 5 hours 17 minutes
Hour eleven, the screen said 5 hours and zero minutes.
That number is supposed to help you understand how long you will wait to see a doctor for a non life threatening condition. Chest pain with difficulty taking a deep breath is a life threatening condition.
In 2016 my late husband was very ill just before New Year's; his O2 levels were 68% (should be close to 100%). The ER waiting room was full; they took him first because he was that close to death.
That is how the system is supposed to work: the sickest people go first, and the waiting time on the screen is supposed to be for everyone else. But what happens when the sickest people are also waiting 13 hours?
I was scared when they took him first, I knew then that he was very ill and might not survive. I vowed then to never complain about wait times because I knew if I had to wait that I was not dying.
Now
I am scared to get sick because we have people waiting hours and hours to be seen and then dying before they can see a doctor. I no longer believe that if I am waiting I am not dying.
England already ran this experiment
It started the same way it is starting here. A government looking at the public health system and saying "it is too expensive, it is inefficient, we need private sector innovation." They underfunded the NHS for years, froze staff wages, closed beds, and then stood back as the system began to fail. When it failed they pointed at it and said "See? Government health care does not work. We need private options."
Private clinics offered scheduled surgeries for hips, knees, and cataracts, the profitable stuff that does not require overnight stays or trauma teams.
They offered something else too: better hours. No weekends. No night shifts. No hallway medicine. Just nine to five, regular pay, and a parking spot.
Staff left because who would not want a Monday to Friday, 9 to 5 job when working in health care? When the public system must be open 24/7, who would not want holidays off?
That is what happened. The private sector did not create new staff; it stole existing staff from the public system. The public system got the skeleton crew and the hallway chairs and the 13 hour waits.
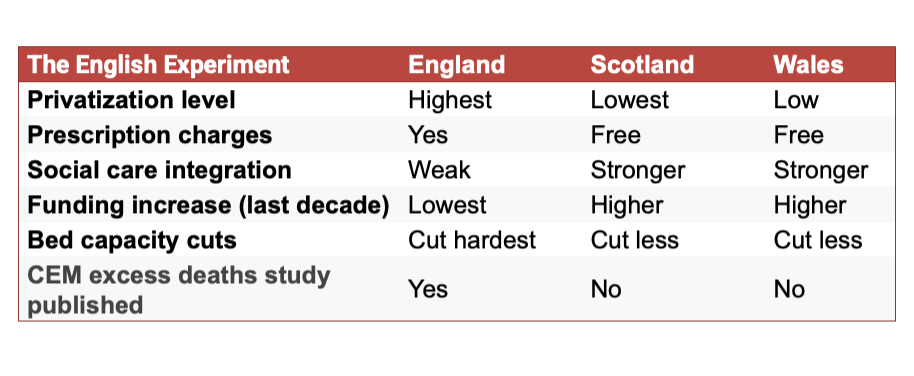
The UK is not one single health system. Think of the NHS like Canada's health care brand: the name is national, but each UK nation runs its own system. England went hard on privatization and competition. Scotland and Wales made different choices: fewer private contracts, free prescriptions, more public control.
The results are not even close.
Created by Kelly Allard - Owl News
Here is the scary part
Dr. Paul Parks has been an emergency physician in Medicine Hat for a long time. He is a past president of the Alberta Medical Association. He has seen every crisis this province has thrown at him. COVID, flu seasons, budget cuts, Code Orange events.
And he has never done what he is doing now.
He is touring Alberta on his own time, with his own voice, volunteering with Friends of Medicare, because he says the system has finally reached a point where staying quiet would be unethical. He shared that story about the 13 hour chest pain wait. He has dozens more.
Now think about the United Kingdom
In England, the Royal College of Emergency Medicine felt compelled to publish a study showing 1,300 excess deaths a month from long A&E waits.
In Scotland and Wales, no such study exists. No royal college there has felt the need to count bodies and sound the alarm like that.
And here in Alberta? No royal college. But we have Dr. Paul Parks. A past president of our own medical association, touring the province, telling stories, begging for change.
England has a body count.
Scotland and Wales have silence.
Alberta has a doctor on tour.
Ask yourself which one looks more like England.
Now 1,300 people a month are dying in England, not from lack of a diagnosis, but from waiting for a bed that never came in time.
The Royal College of Emergency Medicine has the receipts. They published them. And the British government cannot hide from the math.
The Alberta government is reading the same playbook England used. The only difference is that England did not have the advantage of watching someone else fail first. Alberta does. We get to see the train wreck in real time from across the ocean. We get to read the headlines and count the bodies and say "maybe do not do that here."
What does private health care have to do with any of this? Everything and nothing
Here is what Dr. Parks wants you to understand: if you have 50 million dollars in the bank, you still sit in that chair and watch that lying screen tick from 5 hours to 5 hours to 5 hours. There is no private helicopter that lands on the hospital roof and whisks you past the line, because emergency rooms do not work that way.
The private clinics the Alberta government keeps announcing are for scheduled surgeries like knees, hips, and cataracts, the easy stuff and the profitable stuff. They do not handle chest pain, strokes, the 2 AM car crash, or the grandfather with O2 levels of 68%.
When the government takes nurses and doctors and technicians out of the public system to staff those private clinics, who is left in the emergency department? Fewer people, tired people, burned out people. And the patients waiting in chairs pay the price. England already tried this. It does not end well.
The government Keeps Deflecting -Do not fall for it
Every time someone asks about ER wait times, the Premier and her ministers point to private surgical centers. "Look," they say, "shorter waits for hips and knees. Is not that great?" Meanwhile, a 40 year old with chest pain waits 13 hours in Edmonton, and a man named Mr. Sreekumar waited 8 hours in a different ER before dying in that waiting room.
Dr. Parks wonders if any MLA or the Premier would sit in an emergency department chair for 13 hours with chest pain, watching a screen lie to their face. You know the answer: they would not last 13 minutes.
June is supposed to be a slower month for ERs, with wait times usually dropping a bit before the fall and winter crush. If this is the "good" time of year, what happens in November when flu season hits and the usual winter surge arrives?
The government has done nothing concrete to fix this.
Nothing at all.
Just announcements, press releases, and a non binding referendum about a referendum that nobody asked for.
So here is where you come in
You cannot buy your way out of a broken ER, and you cannot private your way out of a hallway. The only thing that works is funding the public system: paying nurses and doctors enough to stay, opening public beds, and treating health care like what it actually is. A basic human right. Not a business opportunity.
England wrote the warning in their own blood.
Alberta read it and said "hold my beer."
Dr. Paul Parks is doing the job the government should be doing: counting, caring, telling the truth. We interviewed Dr. Parks seven months ago. The video has been on YouTube since then. So has the recording of his second tour stop, at the Palliser Friends of Medicare AGM.
Go watch them. They have been sitting there for months, collecting digital dust, while our emergency rooms got worse.
The warning was there. The doctor was there. The camera was there.
The only thing missing was a government willing to listen.
And the next time someone tells you private health care will fix our ERs, ask them one question. If money could buy you out of that chair, why is a 40 year old with chest pain still waiting 13 hours? And why is the screen still lying?
Code Orange over. Go yell at someone who deserves it.
Code Orange over. Go yell at someone who deserves it.
RCEM Report The State of Emergency Medicine in England